
Peptides: The Current Landscape of GLP-1s
Semaglutide vs Tirzepatide vs Retatrutide

This article is for educational purposes only. The compounds discussed are prescription medications or investigational drugs. They are not supplements. They are not FDA-approved for casual use. Nothing here should be taken as medical advice or as encouragement for personal experimentation.
GLP1s for the Mass Market
GLP1-s are the first “meta drug” of the 21st century.
What does that mean?
In this case, Im not referring to their biochemical properties or how they work, but rather their marketing and prominence in the public conscious.
If you’re alive in 2025, you’ve heard the words Ozempic or Wegovy more than a couple times. These aren’t obscure molecules tucked away in diabetes journals anymore. They’re hashtags, punchlines, Wall Street darlings, and front-page news. Serena Williams is marketing it with a billion dollar campaign behind them. Everyone knows someone who is using them.
GLP-1s are going to become Memes, the same way that SSRIs did. But in far less time.
The irony is that GLP1s weren’t supposed to be sexy. They were originally designed to be diabetes drugs, with the purpose of lowering blood sugar in middle-aged patients. Instead, they became the first pharmaceutical to make fat loss not just possible, but probable and possible, and at SCALE.
Ive been unapologetic in my support of them.
The truth is that millions of people who had previously failed diets and gyms for decades suddenly have access to compounds that enable PERMANENT fat loss by changing their cognitive and metabolic chemistry.
But this isn’t another history lesson about how incretins were discovered or how Novo Nordisk engineered semaglutide. We’ve covered that already.
This piece is about the three compounds that matter right now:
Semaglutide – aka Ozempic, the singular GLP-1 agonist that showed what could be possible
Tirzepatide – the dual agonist that one-upped it, and started to make people aware of the power of the compounds for fat loss
Retatrutide – aka “Reta” or “Retard”, the still-experimental triple agonist that bodybuilders and biohackers are already treating like a cheat code.
Each represents a rung on the evolutionary ladder of GLP1s. And if you want to understand where metabolic medicine is going, you must understand how they work, and how they are different.
Semaglutide: The First Breakthrough
When semaglutide landed in 2017 as Ozempic, it was not marketed as a revolutionary drug.
It was pitched as a weekly diabetes drug, basically liraglutide with a better schedule.1 It was regarded as a tool for doctors to help their diabetic patients. It ticked the clinical boxes, for better blood sugar control, fewer jabs, and maybe some cardiovascular health improvements. All the clinical trials had been for diabetes treatment, NOT weight loss/fat loss.
Then the twist hit. Over a few years, physicians began to ntice that the blood sugar levels were not the only numbers plummeting, so too were the numbers on the scale for their patients. And the weight loss was medically significant, in the double-digits. Suddenly, the “diabetes drug” was helping patients lose weight that tried and failed to follow diets previously.
The drug was not without side effects to be sure. To quote directly from wikipedia
Possible adverse effects include nausea, diarrhea, vomiting, constipation, abdominal pain, headache, fatigue, indigestion/heartburn, dizziness, abdominal distension, belching, hypoglycemia (low blood glucose) in people with type 2 diabetes, flatulence, gastroenteritis, and gastroesophageal reflux disease (GERD).[15] It has in the past been suspected to cause pancreatitis, and can cause gastroparesis, and bowel obstruction.[34] Among people who were prescribed a GLP-1, 0.1% were diagnosed with gastroparesis at least six months later, which equates to a 52% increased risk of being diagnosed with gastroparesis while on a GLP-1 medication.[35] A 2019 meta-analysis did not indicate a significantly elevated risk of acute pancreatitis.[36]
Speaking as a Broscientist and what Ive seen in the fitness world, Ozempic by far has the most side effects when compared to Tirzepatide and Reta.
But regardless, Ozempic was delivering on fat loss. By 2021, Novo Nordisk dropped the higher-dose Wegovy, and semaglutide was no longer just a diabetes drug, but being prescribed for fat-loss as well.
Same molecule, but three names: Ozempic for diabetes, Wegovy for weight loss, and Rybelsus for pill-poppers who hate needles. Formal clinical trials for weight loss started in 2021, which is why its so widely prescribed today.
How Does It Work?
Semaglutide works by mimicking GLP1, a gut hormone released after you eat. GLP1 slows how fast food leaves your stomach, boosts insulin, lowers glucagon (the hormone that raises blood sugar), and, most importantly for weight loss, it tells your brain you’re full.
The catch is that natural GLP1 is broken down in about two minutes. That’s useless as a medicine. Scientists modified the molecule so semaglutide latches onto proteins in the blood, shielding it from destruction. The result: a half-life of about seven days. That’s why it only needs to be injected once a week.2
Clinical Trials
In 2025, the STEP UP trial dropped data that pushed semaglutide’s ceiling even higher. Researchers tested a higher 7.2 mg dose of Wegovy in adults with obesity (no diabetes), and the results were staggering: an average 21% weight loss over 72 weeks.
Over 90% of participants lost at least 5% of their body weight, and a third lost 25% or more. For context, that kind of number is usually reserved for bariatric surgery, not a weekly injection. The side effects were mostly the same GI issues already familiar with sema, and only 3% of people dropped out because of them.3
But there were ISSUES. Some patients stalled out at around 15% weight loss, and the higher dosing did lead to more side effects, even if people didnt drop out the study.
At the same time, there was another drug that had already hit the market and was proving superior to Ozempic, from a rival Pharma company.
Tirzepatide: Dual action
If semaglutide cracked the door, tirzepatide kicked it off the hinges. Approved for diabetes in 2022 under the brand name Mounjaro and in 2023 as Zepbound for obesity, this drug made Ozempic outdated. As fast as it appeared, there was already a better alternative on the market .4
How It Works
Tirzepatide is a dual agonist. Like semaglutide, it works on GLP1. But it also activates GIP, another incretin hormone. On its own, GIP never looked impressive. But when paired with GLP1, it changes the game. GLP1 suppresses appetite and controls blood sugar.
Its still one molecule, but its attaching to two receptors. Early on, many doctors questioned whether that added second pathway would add anything useful. But the trials shut down the skepticism.5
GIP seems to boost insulin sensitivity and improve how the body handles fat. The result is a metabolic tag-team effect: one partner suppressing appetite, the other optimizing nutrient partitioning through increasing insulin sensitivity.
Clinical Trials
This global phase 3 trial enrolled more than 2,500 adults with obesity (but without diabetes) and tracked them for 72 weeks on once-weekly tirzepatide. The results weren’t subtle. At the top 15 mg dose, people lost an average of 21% of their body weight, nearly ~49 pounds on average.
Even the lowest dose, 5 mg, delivered a 15% reduction, far beyond what older obesity drugs ever managed. Around 90% of participants hit the basic 5% weight-loss mark, and about 36% of participants lost 25% or more of their body weight.
That’s surgery-level territory, achieved with an injection. And it wasn’t just the scale moving. As from the shrinking waistlines, there were the improvements in blood pressure, improvements in A1C, and over 95% of participants with prediabetes returned to normal blood sugar.
The side effects were mostly nausea, diarrhea, and constipation, the same GI issues seen in the semaglutide group, but the dropout rates were low, and side effects a bit less prevalent. The New England Journal of Medicine called the results “unprecedented,” and it wasn’t hype. It was the establishment admitting the obvious: this was the first time a drug looked like a true competitor to bariatric surgery. 6
Retatrutide: The Triple Agonist and the Underground Favorite
Retatrutide is a triple agonist, it works by flipping three switches at once. GLP-1 and GIP are gut hormones that tell your brain “you’re full,” slow the stomach down, and help the pancreas handle sugar. The third, glucagon, looks weird at first because it can raise blood sugar.
But in this combo it also nudges the body to burn more energy. And store less glucose in the liver. And improves lipid markers. And increase fat oxidation. And has the effect of reducing fatty liver disease. And at the right dose seemed to slightly raise metabolic expenditure. And also people lost more weight than compared to Ozempic and Tirzepatide.
If those effects sound too good to be true, it is why the early results turned heads.7
In a 2023 phase 2 study, people on the highest dose lost about 24% of their body weight over 48 weeks (roughly one quarter of their starting weight). They didn’t just get lighter: liver fat dropped, insulin sensitivity improved, and heart-risk numbers moved in the right direction. If the larger phase 3 trials repeat that pattern, retatrutide will set a new high-water mark for medical weight loss.8
Outside the clinic, the story’s messier.
Biohackers and many physique athletes are already using Retatrutide widely, as are Techies in Silicon Valley. In the world of research chemicals, its widely available.
This has led to an interesting situation: a drug designed for people with obesity is getting applied and studied by more fit populations, who are pioneering its practical usage and how to optimize its effects, but its not yet on market as a prescription drug.
The side effects look familiar compared to the predecessor GLP-1 drugs: nausea, vomiting, diarrhea or constipation, but at a lower frequency. In the Biohacker world, Its generally regarded as having the most minimal side effect profile.
The two side effects that do stand out are more stimulatory; some people experience an increased resting heart rate (although this is reported to fade away after the first month), and some report difficulty sleeping more than 5-6 hours.
Biohackers gonna biohack. These effects are attributed to the glucagon is in the mix, as trials have also picked up small bumps in heart rate. Whether that’s harmless or a long-term concern isn’t known yet, no one has a decade of follow-up. That uncertainty hasn’t stopped early adopters, but its also why regulators move slower.
If phase 3 stays on track, Retatrutide will finally hit the market as as prescription drug in 2027. So the general public will learn about in 1.5 years, and meanwhile the cutting edge people will figure out the real world application.
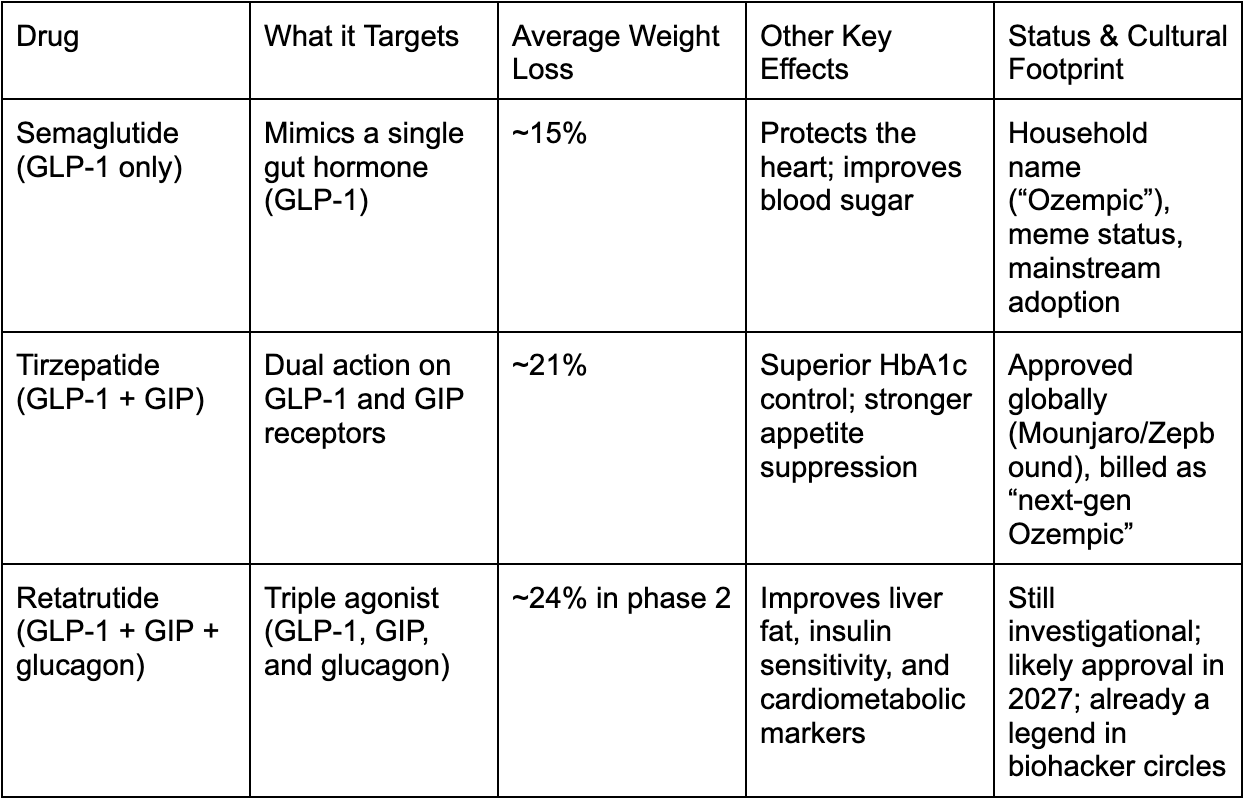
Comparing the Big Three
Here’s how the hierarchy shakes out:
The Metabolic Land Grab
The obesity drug race is not ending with Reta though, as now Big Pharma companies are chasing the next wave: combo agonist, orals for people who dont want to inject once-monthly shots for convenience, and trying to combine Incretins with myostatin inhibitors to spare lean mass.
Fat loss+metabolic improvements+lean mass preservation=
2027 is the obvious tipping point, the year Retatrutide is expected to break out of trials and hit the mass market. DelveInsight flags it among nine horses to watch by 2030, a short list of contenders rewriting what obesity treatment looks like.9
The strategy for all companies is clear: stack the hormones, widen the effect. Duals and triples are going to become quadruples and quintuples eventually.
The Biohacker Underground
In the depths of biohacker world there are already people combining GLP-1 with GIP and glucagon agonists, AND adding in amylin agonist, AND stacking that with growth hormone secretagogues, mitochondrial small molecules, and in some cases TRT. Or in the case of bodybuilders, Full steroid cycles.
Thats CRAZY.
Yes it is. And if you are in those community, there are before and afters that defy belief. And its not crash dieting either. People are achieving permanent fat loss while getting in the best shape of their lives.
In the biohacker and bodybuilding world, GLP-1s aren’t seen as medicine, rather they are described more like tech. Semaglutide is seen as Gen 1, tirzepatide as Gen 2, and retatrutide as Gen 3.
Officially, retatrutide is still locked in the TRIUMPH trials, but just like with other peptides, the underground world is already experimenting as if the launch has already happened. Semaglutide (Ozempic) was used back in the 2016 by bodybuilders a full year before it came to market. Tirz and Reta are no different. Inside these communities, the drug’s “abilities” often get described like a Marvel power list instead of a pharmacology chart, and Reta is King:
Strip fat while sparing muscle
Boost insulin sensitivity to “cheat” carb loads
Flatten visceral belly fat faster than sema or tirze
Improve liver health and lipid profiles as a side bonus
Increase calorie burn through glucagon’s thermogenic kick
Potentially enhance endurance by lightening metabolic drag
The risks don’t go unmentioned though, and ironically this user base has far more experience with controlling side effects and optimizing usage. Regardless, its firmly DYOR (Do Your Own Research) if you venture into that world.
To Learn More About Biohacking you can Join my Free Community on Telegram
References:
Kommu, Sharath, and Philip Whitfield. “Semaglutide.” StatPearls, StatPearls Publishing, 2025. PubMed, http://www.ncbi.nlm.nih.gov/books/NBK603723/.
“How Does Semaglutide Work?” Mayo Clinic Diet, https://diet.mayoclinic.org/us/blog/2024/how-does-semaglutide-work/. Accessed 7 Sep. 2025.
James, Davy. STEP UP Trial Shows Higher Dose of Wegovy Produces Significant Weight Loss in Adults With Obesity Without Diabetes | Applied Clinical Trials Online. 7 Sep. 2025, https://www.appliedclinicaltrialsonline.com/view/wegovy-weight-loss-obesity-diabetes.
Farzam, Khashayar, and Preeti Patel. “Tirzepatide.” StatPearls, StatPearls Publishing, 2025. PubMed, http://www.ncbi.nlm.nih.gov/books/NBK585056/.
SURMOUNT-1 Study Finds Individuals with Obesity Lost up to 22.5% of Their Body Weight When Taking Tirzepatide | American Diabetes Association. https://diabetes.org/newsroom/surmount-1-study-finds-individuals-%2520with-obesity-lost-up-to-22.5-percent-body-weight-taking-tirzepatide. Accessed 7 Sep. 2025.
Jastreboff, Ania M., et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, vol. 387, no. 3, Jul. 2022, pp. 205–16. DOI.org (Crossref), https://doi.org/10.1056/NEJMoa2206038.
Abdul-Rahman, Toufik, et al. “The Power of Three: Retatrutide’s Role in Modern Obesity and Diabetes Therapy.” European Journal of Pharmacology, vol. 985, Dec. 2024, p. 177095. ScienceDirect, https://doi.org/10.1016/j.ejphar.2024.177095.
Jastreboff, Ania M., et al. “Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial.” New England Journal of Medicine, vol. 389, no. 6, Aug. 2023, pp. 514–26. DOI.org (Crossref), https://doi.org/10.1056/NEJMoa2301972.
Joshi, Sandeep. “9 Obesity Drugs to Be Launch by 2027.” DelveInsight Business Research, 12 May 2025, https://www.delveinsight.com/blog/obesity-drugs-launch.
Have you had any clients using orforglipron with any success?
My compounding pharmacy just notified me that they are unable to compound Sema it Tirzep. They offered me Liraglutide? Any info on that?