
The Broscience Guide to Testosterone Replacement Therapy 2025 Edition
by AJAC

A Table of Contents:
0) Introduction
1) Testosterone, the Male Hormone
2) Why Raise Your Testosterone At All?
3) The Testosterone Collapse
4) Testosterone Decline and Levels Over a Lifetime
5) Total Testosterone and Free Testosterone
6) How Does TRT Work? (Prescription and Basic Usage)
7) Optimizing TRT Experience
8)The Most Common TRT Questions
9) Recommended Resources
FYI-This article has been updated since I first published it 3 years ago. It is lengthy and take your time reading it.
0) Introduction-Testosterone, the Male Hormone
TRT, shorthand for Testosterone Replacement Therapy, is the subject of much speculation, uncertainty, and “disinformation” to use the term. This article is my attempt to dispel the mythology and provide a practical and evidence-based overview, understanding, and relevant actions to take.
Everything in this article is supported by the most recent medical research and accumulated anecdotal evidence. Where I engage in bro theorizing and speculation, I explicitly make note of. Many sources are included.
To preface further, I am not an MD or DO. I do not work in a clinical laboratory. I am not on TRT, which no doubt some people will consider disqualifying immediately. Thats fine, you can exit now.
My experience with TRT is in the realm of professional experience; I have worked with clients on TRT and full steroid cycles for over a decade. I am familiar with clinical ranges and what numbers mean. I have seen how they change, both with natural intervention and with exogenous intervention.
This has required me to educate myself on how it works, and to be able to answer the questions and make suggestions when appropriate.
It has been my experience that many physicians have a poor understanding of male hormones and the HPG axis, and even prescribing doctors will give advice that runs counter to physiology.
This is what led to create resources for clients, and what has evolved into the article you are reading.
It is my belief that every Man should be knowledgeable of his health and be empowered to make the best decisions possible that give him the greatest quality of life.
You should not be ignorant of the functioning of your own body. You should understand what “blood work” means. You should know what biomarkers and lab tests are relevant (although for the sake of specificity, we will stick to testosterone in this article).
Ultimately, your decision to use or not use TRT is a personal one, and will likely require oversight from a medical professional. Per legality, listen to the medical professionals. Or at least pretend to. Everything in this article is for your own education.
1) Testosterone, the Male Hormone
To quote wikipedia “Testosterone is the primary sex hormone in Men”.
Testosterone is an androgen, belonging to the class of hormones called Androstanes. It is synthesized in the testicles from cholesterol (cholesterol intake is beneficial for testosterone production). As the primary sex hormone, it has what is defined as androgenic/anabolic properties. Testosterone is a growth hormone. Muscle, bone, tendons, collagen, and hair being obvious examples. Testosterone is what masculinizes men and makes them sexually dimorphic from women.
Unlike women, who generally have some intuitive understanding that hormones play a role in their health by way of their menstrual cycle and its fluctuations, Men tend to NOT think about their testosterone levels at all, until it becomes an issue.
If you are redpilled on health, as the phrase goes, you likely have some idea that testosterone levels matter, are critical to feel healthy as a man, and you are probably interested in elevating them and/or maintaining them.
This is uncommon. For many millions of men, testosterone levels are not something they consider until they first learn of their T-levels in their 30s or 40s or even later. Maybe a doctor recommends they get tested as part of a physical. They have no clue what the numbers mean. They attribute their low energy, lack of libido, and general decline to “aging”. That the culprit is hormonal is not taken seriously, let alone thought of.
Testosterone deficiency is NOT a new phenomenon though. As far back as 4000 years ago, in both Ancient Greece and in Ancient China, there are historical records documenting the practice of castration in both animals and in Men.
As barbaric as this is today, it does give insight into human observation and natural scientific thinking.
The Ancients in these cultures recognized that the testicles produced SOMETHING that made men and male animals aggressive, independent minded, sex driven, and combative. By way of castration, the resulting eunuchs were much more docile, and considered obedient and easier to control.
While it would be millennia before testosterone was isolated and discovered, the ancient world did attempt its own version of “testosterone enhancement”, largely through ingestible concoctions of animal testicles. Whether these concoctions worked on it is not well documented, but an effect is possible. Regardless, it is evidence that Men have been attempting to elevate their vital energy for a very long time.
Testosterone the hormone remained unknown for centuries, and it was not until 1889 that the scientist Charles Edouard Brown Sequard injected himself with a mixture of his blood, semen, and “juice” from animal testicles (possibly dogs or monkeys or guinea pigs) that that the concept of direct injection arose in science.
Brown Sequard claimed that he had experienced increased energy and libido from these injections, and administered them to thousands of men as well.
-To note, do not attempt this at home. Modern science discovered that while testosterone is made in the testicles, it is NOT stored in the testicles, and for Brown Sequard's experiments to work, he would have needed the equivalent of about 1000lb of animal testicles for ONE injection. Unless there is some other mechanism that took place, his experiments were likely a placebo effect.
Brown Sequard was considered eccentric and his experiments were considered dubious, but they did ignite wide spread research on discovering the testicular secretion responsible for the purported effects.

Finally in 1929 the German biochemist Adolf Butendant isolated testosterone from human urine.
And in 1939 the Croatian scientist Leopold Ruzick synthesized testosterone for medical usage, which contributed to his winning the Nobel Prize for Chemistry.
With the ability to synthesize testosterone, the era of Hormone enhancement in Medicine had begun. The world would never be the same.
2) Why Raise Your Testosterone Levels at All?
So now you know the history of testosterone. But why elevate it? The reasons are clear.
As the primary androgenic sex hormone responsible for masculine sexual characteristics. It makes Men, MEN.
Cognitively, testosterone increases mental focus, memory retention, motor coordination, perceived sense of well being, and has the obvious effect of increasing sexual libido.
Structurally, testosterone affects muscle growth, muscle recovery, muscle density, and muscular force output. Testosterone improves strength across all levels, from low intensity to high intensity.
Testosterone increases bone density, accelerates collagen production, and improves recovery.
Having high testosterone levels in combination with physical fitness is a feeling of immense physical power. Men who are in this peak hormonal and physical shape can attest to the feeling.
Being testosterone deficient is essentially the opposite of living with Vitality.
The Symptoms of Low Testosterone
My first encounter with a Low testosterone client was in 2011. I had a Korean gentleman in his early 40s who came to me concerned about why he was not getting stronger.
He was doing all the right things in regards to training and diet. He lifted 3-5 times a week, did daily cardio, and his diet was clean (whole foods and he did not consume much sugar or drink alcohol). He slept okay, but he felt there a lack of energy, drive, and strength that should be there, but was not.
He was frustrated with his lack of results, and I suggested he get his testosterone levels checked.
About a week later he returned, thanking me profusely. His total testosterone had been less than 300, and he was diagnosed as Hypogonadal (testosterone deficient). He was given a prescription for Testosterone Replacement Therapy.
A few months later, he had transformed. He had gained 10lbs of muscle, was leaner, much higher energy, and he reported to me he felt the best he had EVER felt in his life. Such was the power of optimized testosterone levels.
3) The Testosterone Collapse (Alex Jones was Right)
In the 20th and into the 21st century, there has been a societal decline in testosterone levels in American men. This is not solely confined only to America, but has been seen in other countries, and even seen in animals as well.
As Alex Jones infamously said “they are turning the frogs gay!”
Directionally speaking, he was not wrong.
The Frogs are not turning gay, rather the frogs are turning into girls.
So are the Fish.
This decline is also independent of the normal decline associated with aging. It is factually true that testosterone decreases as men age, but the decline seen today is not only in older men, but men in all age cohorts. There are a multitude of studies documenting, the following are some of the most relevant ones.
Testosterone Levels Decreasing in Danish men
A Population-Level Decline in Serum Testosterone Levels in American Men (this is where the 1% year over year decline statistic comes from)
1 in 5 adolescent and young adult males has testosterone deficiency.
In this study, 38.7% of men over the age of 45 were hypogonadal (testosterone deficiency)
It is not fear mongering to say testosterone levels are declining, the scientific evidence validates this trend many times over.
To make sense of what testosterone decline means, we need to examine what normal testosterone levels are.
This is where we get to the numbers. Pay close attention. Depending on the country you are in, the units of measurements will vary. I cover examples below, and by the end you should be able to make sense of your own blood work no matter where you live and how it is measured.
4) Testosterone Decline and Levels over a Lifetime (and making sense of Bloodwork)
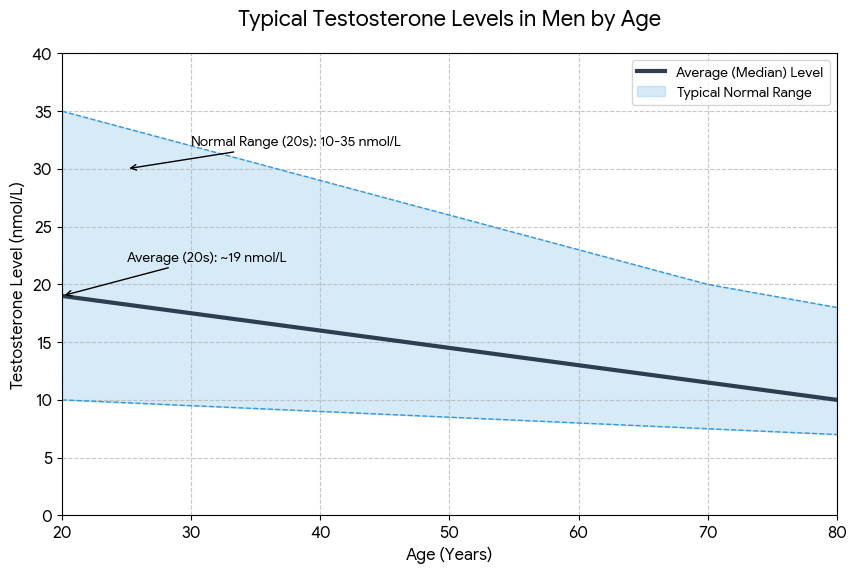
Let us start with this chart.
Newborn boys experience a testosterone surge in the first few months of life, which quickly subsides. It is not until a boy experiences puberty that his body will produce significant levels of testosterone again.
This chart shows the total testosterone levels for each age bracket, up until age 40.
You will notice these numbers are given as a RANGE.
Your testosterone levels will fall within an average statistical distribution for your age bracket. As you can see, the ranges are quite large. Supposedly normal testosterone levels for age 18-39 are apparently anywhere from 300-1080 nanograms per deciliter.
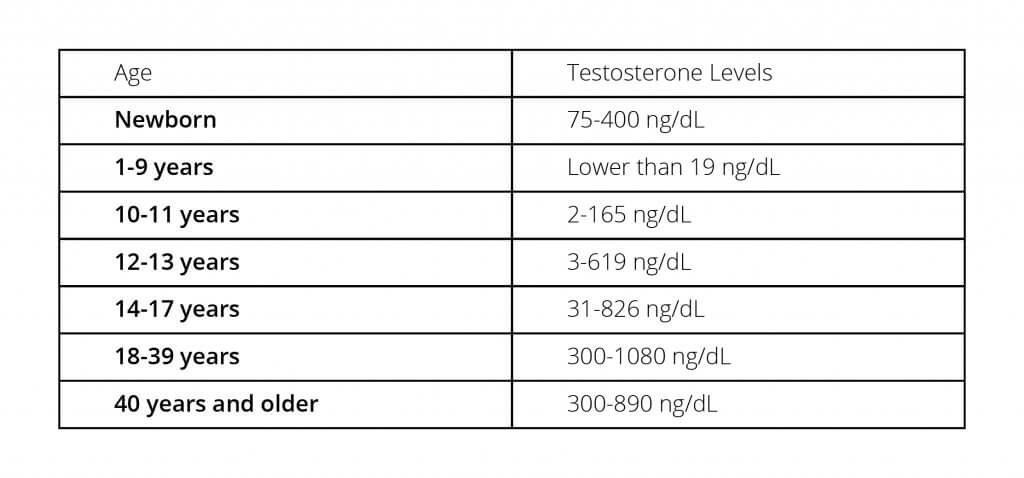
That these ranges are so large is why determining low testosterone levels is confusing. Defining normal as anywhere from 300-1100 does not help us much.
To make sense of this, we need to look at the statistics for what the median and mean levels are in each bracket, not just the range of distribution.
In this chart, based on the data of 1,185 normal weight men, ages 19-39, we can see how testosterone levels are distributed. The upper 5% of men have levels over 850 in total testosterone. The top 50% of men have levels over 531, while the bottom 50% have levels under 500. 10% of the men have levels of 349 or lower.

The results of this study are fairly typical and match up with other collections of data; 500 is about the median level for men ages 18-40.
If we examine average levels for more precise age brackets, we get further insight.
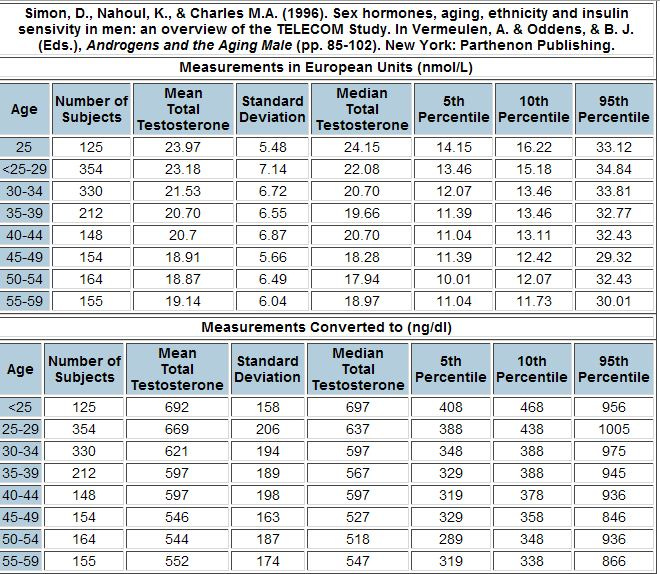
This data is taken from the TELECOM study . It shows the MEAN testosterone levels for each age bracket. The data is presented in both nanomoles per liter (a common way of measuring testosterone in Europe), and nanograms per deciliter.
For men 25 and younger, the MEAN levels were 692 ng/dl in total testosterone.
For men 25-29, they were 669 ng/dl .
For men 30-34, they were 621 ng/dl .
Even in men who were 55-59 years old, Mean testosterone was 552 ng/dl. Interestingly enough, the Mean was higher in the 55-59 year old than 45-54 year olds. These numbers also clearly show that men in the bottom 10% of testosterone levels all have total Testosterone of less than 500.
Up until the 1990s, having total testosterone levels of lower than 500 was the “average” only in 70+ year old Men
The historical evidence supports an approximate average testosterone level of 500 for men even up to age 65-74. .
This is why TRT clinics generally have considered 500 as the consideration point for a man being a candidate for Testosterone Deficiency.
The above data is older data from the 1990s. In the last decade average testosterone ranges have changed
In 2017, a new Study Defines Normal Ranges for Testosterone Levels
This study took 9,000 American and European men, looked at their testosterone levels, and crunched the numbers. These numbers were then used as the updated reference range.
In an insidious bit of statistics, the new “normal” range was notably lower than the old normal range.
The harmonized normal range for testosterone in a non-obese population of European and American Men, 19-39 years, is 264-916 ng/dL.
For context and comparison, the old range (which did vary somewhat depending on organization) generally defined 300-350 as being low normal, and 1000-1200 ng/dl as high normal.
You see the problems here?
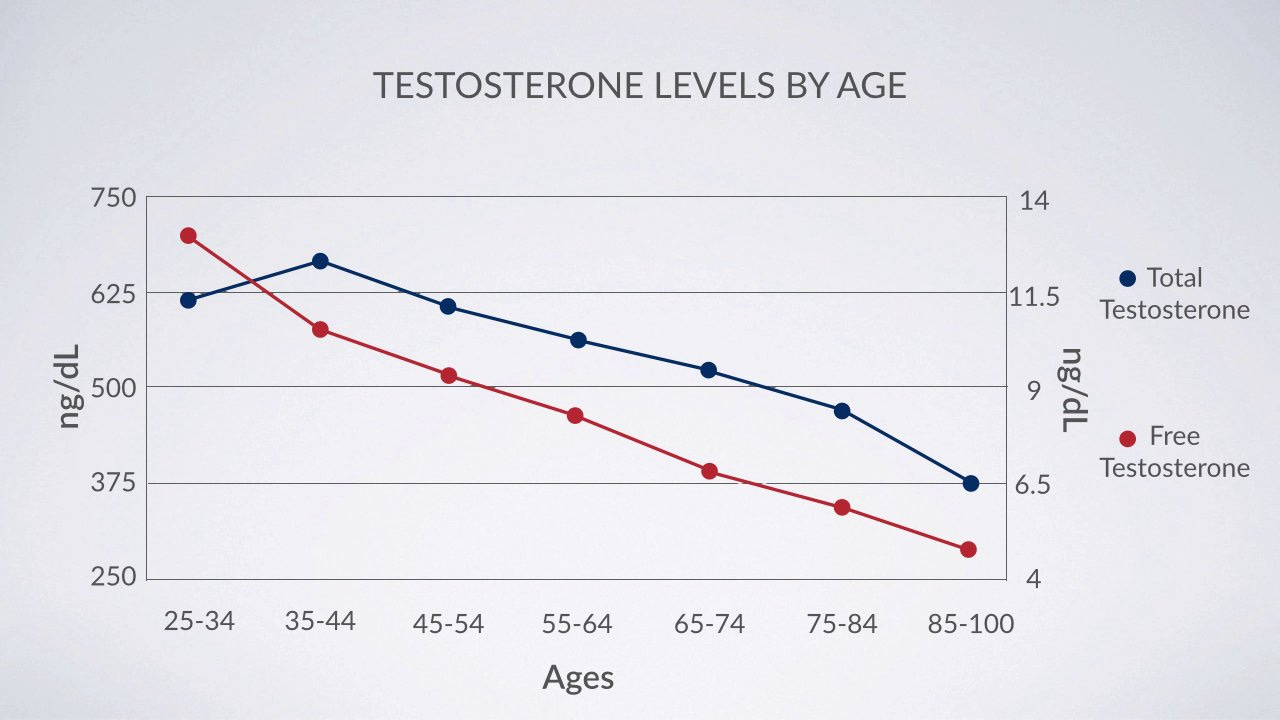
Testosterone levels on average decline by about 1% every year after age 25. But normal testosterone levels have also declined every year since the 1980s in American men. What is considered “normal” is trending lower year by year.
In 1987-9189, the median testosterone level in men who were ages 45-71 was 501.
In 2002-005, it was 391.
Again, this decline in testosterone levels is independent of normal aging. The 45 year old men who are testosterone deficient in 2022 quite likely had “low normal” levels when they were 25, but unless they got tested, they have no idea what their levels actually were.Based on historical and current data, we can infer that the lower your testosterone levels are when you are young, the lower they will inevitably be as you age. If your levels in your early 20s right now and are already “median” to low normal then, you need to prioritize getting those levels UP.
Statistically, 1 in 5 teenagers and young men under the age of 24 are Testosterone deficient.The overwhelming majority of primary care doctors will never actually look at historical ranges, means, medians, age brackets, or standard deviations. They will look at the range, and if you are in “normal range”, you are FINE. And that is it. End of discussion.
This new reference range then is based on data from men who in all probability had LOWER testosterone than the average man from 30, 20, even 10 years ago. So we are making up new numbers taken from low testosterone men, and calling that “Normal”.
Rather than address the testosterone deficiency, Big Medicine elected to simply lower the standard ranges to accommodate the decline.
AJACs Bro Perspective-Most Primary Care doctors are uninterested in health optimization, and have minimal education in testosterone therapy. Doctors are trained to treat disease, not promote health.
There is a distinct probability they will discourage you from getting your testosterone levels tested, you will be told there is no point to doing this, and in the event you do get the blood tests done, they will tell you your testosterone is normal unless your total testosterone is under 200 and you explicitly state your penis does not work, you cannot get an erection, and you feel depressed.
And even then, you will probably be discouraged away from TRT, and pushed towards Viagra or Cialis.
You will also be told TRT causes cancer, prostate cancer, cardiovascular risk, makes you permanently infertile, and may even be told it doesn't make that much of a difference (all of this is clinical grade dogshit as we will get to later)
Rarely does any man have a positive experience when he inquires into his testosterone levels with his doctor.
Maybe 1 in 4 doctors is open to the idea and has useful advice for the patient and can explain what the numbers even mean beyond “they’re in normal range, you are fine”.
5) Total Testosterone vs Free Testosterone, and How It All Gets Measured
I get the question weekly from Men who have their testosterone levels, and then contact me asking “what do these numbers mean?”
By this point, you should have an understanding that testosterone levels are measured within a given range, and where you fall within that range relative to your age is what matters.
In America, the most popular way to measure testosterone is using a total testosterone test, which is measured in nanograms per deciliter. This is shown as ng/dl.
Total Testosterone
This is basically all the testosterone molecules floating in the blood at any given time. This includes bound and unbound testosterone molecules. Bound testosterone means the testosterone molecule is biochemically attached to sex hormone binding globulin (SHBG), albumin, or cortisol.
Your total testosterone will be compared to the reference range, which will likely have 200-300 as the low end, and 900-1100 as the high end.
Under that there is no completely standardized exact reference range that is universally used everywhere. But they are all highly similar, so it does not matter. How your doctor interprets it matters much more.
Free Testosterone
At any given time, only 1-2% of the testosterone in your body is “bioavailable”, meaning it is unbound and can act on any androgen receptor anywhere in the body. It is this free testosterone that drives the anabolic effects of muscle building and tissue regeneration.
This bioavailable testosterone is measured as “Free Testosterone”.
This measurement can be confusing, because it is sometimes measured differently from total testosterone. It can be shown as ng/dl, or pg/ml, or nmol/L.
The standard ranges also vary much more than that total testosterone range. To simplify though, higher Free T is always better. Whatever your particular range your blood test uses, you want your Free T levels to be in the middle of the range or higher.
The range I see most often in the USA:
46-224 pg/ml.
How do you Know if Free Testosterone is Low?
Unlike Total T, Free T is a little less clear due to the variety of ranges used. Whatever the numerical range on your report, low Free T will usually be regarded as being in the bottom quarter of the given range (or below the range entirely if your free T is extremely low)
Both Total and Free Testosterone are important, but they must be understood in context.
-If you have medium to high total testosterone levels, it is likely that your Free testosterone will be normal as well. (medium being defined as 500 and above)
Occasionally you can have men with healthy testosterone levels, but their FREE testosterone is LOW. When free testosterone is low, SHBG will be elevated.
In this situation, TRT is not automatically the answer. SHBG can be lowered through supplementation (Boron, Magnesium, Stinging Nettle root can all have SHBG reducing effects).
-In contrast, if your FREE testosterone is high, it is unlikely you need TRT, even if your Total Testosterone is not exceptionally High along with it.
In Europe, the measurements are shown differently
Total testosterone and other blood tests are often measured as nanomoles per liter, nmol/L.
This is not a completely different test, it's simply a different way of measuring. If you use the metric system, you should be familiar with powers of 10 and know that numbers can be converted up or down to different units.
You can convert nmol/L to ng/dl (along with a number of other metric measurements) using this handy online calculator.
Dont be helpless people
6) How Does TRT Work? (Prescription and Usage)
Before we dive into this, I want to dispel some common confusion, and answer the question “is TRT steroids?”
This is something of a semantic argument . There is not any such thing as “TRT testosterone” and “steroid testosterone”. They are not magically different. Testosterone is defined as an Anabolic Steroid. You are raising your levels through external (exogenous) means.
Typically in testosterone treatment you will be given testosterone in the form of injections, gels, or creams.
The injectable version of testosterone is no different than what a man would use during a “steroid” cycle. The difference is in the DOSAGE.
A typical TRT dosage given as an injection is generally between 100-200mg a week. A “steroid” cycle of Testosterone is typically 500mg weekly, with dosage up to 1000mg a week being common among hardcore bodybuilders. In addition there are other anabolic compounds that will be taken.
So while you are using anabolic steroids, your dose is likely to be 1/10 to 1/5th of what a bodybuilder would use.
Does being on TRT mean you are on “steroids” then?
Yes or No, depending on who you ask. To repeat, it's a Semantic argument.
This said, if the idea of using sTerOiDs is horrifying to you and triggering, please stop reading and Fuck Off.
I have zero interest in making a moral argument to overcome anyones bitch ass sensibilities surrounding “fairness” and what is “natural”. I cannot help that you are naturally a simpering bitch who clutches your mothers pearls.
The Primary Purpose of Testosterone Replacement Therapy is to Optimize Your HEALTH through optimizing your testosterone levels.
This is the major difference between steroid-level dosages and TRT dosages.
On TRT, the goal is to elevate your testosterone level to high normal ranges. A responsible and informed physician will typically seek to get total T-levels above 700 and usually no more than 1200+, which is the range where Men experience a noticeable difference in energy, well being, libido, and the other aforementioned qualities.
Some doctors will allow patients to venture close to the 1500 range. While you will likely enjoy increased muscle building and strength and fat loss effects, at those levels you may begin experiencing unwanted side effects (high blood pressure, elevated LDL, elevated Red blood cell count, acne, hair loss, etc).
A TRT dosage is only as High as NECESSARY to restore what your body is no longer producing and take you into a healthy high normal range.
This range is usually defined as 700-1200 (give or take 100 points).
A Bodybuilder does not care about “health”, their primary motivation is building as much muscle as possible. Their supraphysiological dosages are thus much higher than what a responsible TRT dose would be.
Their health suffers accordingly, bodybuilders dying young has been a phenomenon since the 1990s.
What Should YOUR Levels be on TRT?
There is no exact answer for this. You determine someones treatment based on their SYMPTOMS, not their mgs.
So now that we got that out of the way, we circle back to how TRT Prescriptions Work in Practice.
If you live in the United States, you cannot simply walk into your doctor's office and ask for testosterone. If you live in Mexico or other Latin American countries (and much of Asia as well) you can readily purchase testosterone and other anabolics over the counter, but let's pretend everyone reading is American for the time being.
To Qualify for TRT, you Need to be showing Symptoms of Low T
Typical symptoms are
-Chronically Low energy and lack of motivation
-Increased fatigue
-Anxiety and low-grade depression
-Lack of libido
-Weak to no erection, or inability to sustain an erection
-Muscle weakness and inability to build strength and muscle
-Slower recovery from physical activity
Feeling Unmotivated or Having Low Energy does NOT automatically mean you have Low T
I have frequently had young men in their 20s contact me thinking they need TRT. They say they have low energy, lack motivation, and believe they are not getting results in the gym.
I always tell them to get tested, otherwise it's all speculation. I'd estimate that at least 2/3rds of the time, their testosterone levels are NORMAL.
They are not high normal 900+, but their T-levels will be in the 500 range or higher.
Their issues are not their hormones, but their mindset and lack of discipline. Following a program, eating healthy, applying themselves to a Mission, competing…they have numerous areas of life that could be improved and would elevate their natural testosterone production.
If you suspect you are Hypogonadal, you need to be showing symptoms for at least 6 months, and have Low T levels on a Blood test
How low is low? As you’ve learned, this depends on your doctor.
In Anti-aging medicine, testosterone levels about 700 are considered optimal, and 500 is the threshold for being considered a candidate for TRT.
Below 400 though, and most any Anti-aging/TRT clinic would likely give you a prescription.
At the 400-500 range, you could conceivably improve your T production through natural means. For men under the age of 30, I ALWAYS recommend using natural and supplemental means to raise testosterone. TRT should be a last resort only if you are suffering and other interventions have not worked.
I have an entire article on this subject.
You Can Ask Your Doctor for a Blood Test without Showing Symptoms…
But do not insinuate that you hope your levels are low so you can get TRT.
Be very clear that you want to be informed about your internal health. Whether your doctor accepts your request will be hit or miss. As said before, doctors are often unwilling to order the tests at all. If that's the case, you will need to pay for them yourself out of pocket.
Moving on, You go to your doctor, express you have symptoms of Low-T, and they order you a blood test.
The Blood test at minimum will include total testosterone. It may not include free testosterone, this you would need to ask for. You want to
It MAY include Cholesterol levels, triglycerides, SHBG, estradiol, and FSH. Your doctor may elect to order a number of tests. Or they may not.
As you will inevitably discover, there is No standard procedure of practice
Some primary care doctors may send you to an endocrinologist, some will not. Some may refer you to an anti-aging clinic. Some will not. Often they will order the tests themselves, or you will be referred out.
You will Need to be Your Own Best Advocate for Treatment
At minimum, you need to know your total testosterone, free testosterone, and SHBG. If total is low, or SHBG is high and free is low, or even if all 3 are low, you will be given enough information to figure out next steps.
Side Note-How to Order Blood Test Yourselves
I recommend Vanguard Labs, order their Total Male Panel (use code AJAC10 for a discount)
Finally, your lab test comes back. Your total testosterone is LOW, say under 300. You have had symptoms of LOW T for Months.
Now what?
Depending on your numbers, and depending on the doctor, different recommendations will be made.
Testosterone Gels-These gels are most popular with lazy doctors who are not educated on TRT. They come in different concentrations. The first generation gels were very irritating to the skin, the new ones are not. This method is not as precise as injections because you have to control how much gel you pump out and apply to the skin. Usually the gel is applied to the shoulders and upper torso. The gel can also be spread by skin to skin contact, so do not apply this to your body and then hug your wife or girlfriend bare chested.
Testosterone Injections-This means using needles. Traditionally injections were done once a week, and they are self administered. Injections are usually done in the glutes, although in theory you could inject any muscular area of the body.
The needles used for these injections can be quite small, and learning how to inject yourself is quite easy, despite the fear mongering around it.
In current practice, injections are best done twice a week to mimic a more natural rise and fall of testosterone. Depending on the type of testosterone injected, injections could be every other day, or even every day.
Injectable Testosterone is the best form, and allows you precisely manage your lab markers and have objective data on your dosage.Testosterone Creams-this is a relatively new form of application. It is a custom made compounding cream applied directly to the Scrotum. Yes, you are putting lotion on your balls.
This application does work testosterone, but for obvious reasons many men would rather inject weekly rather than be lotioning their ball sack daily. It has the same issues as the T gels in not being precise (and also messy).
7) Optimizing Your TRT Experience
I want to directly credit BowTiedHRT for this section.
He is my number 1 recommendation for men looking for TRT consultation and coaching, send him a DM
Being on TRT is not passive, you must become an active manager of your health and there are multiple lab markers you must pay attention to.
While your daily symptoms tell you if the TRT is working, the other biomarkers tell you how your body is handling it, and what adjustments need to be made.
Especially in regards to Estrogen, many side effects men experience of TRT are symptoms of elevated estrogen, and/or elevated prolactin, or potentially too LOW estrogen if anti-estrogen medications are being used.
The IDEAL level of estrogen is unique to the individual
Some men aromatize heavily and their estrogen levels increase faster than others. Some men are much more sensitive to the effects of estrogen, and their ideal level is lower than would be expected.
You can ever assess solely off of numbers, you must incorporate symptoms, quality of life, mood, mental health, sexual performance, and use that to inform your calibration
When you are on TRT, you are essentially manually operating a system that your body used to run on autopilot.
CMP (Comprehensive Metabolic Panel)
What it is: A check-up on your body’s chemical balance and fluid levels.3
The TRT Focus:
Kidney Function (Creatinine / eGFR): TRT can raise blood pressure, which stresses the kidneys. You want to ensure your filtration rate remains high.
Liver Enzymes (AST / ALT): While injections rarely stress the liver, oral testosterone or other added compounds can. This ensures your liver isn’t inflamed.
Electrolytes: TRT can cause water retention; this panel shows if your sodium/potassium balance is off
CBC (Complete Blood Count)
What it is: A broad inventory of your blood cells (red cells, white cells, platelets).
The TRT Focus: You are looking specifically at Hematocrit and Hemoglobin.
Why it matters: Testosterone signals your bone marrow to produce more red blood cells.2 This increases the oxygen-carrying capacity of your blood (good for endurance), but if it goes too high, your blood becomes thick like syrup (polycythemia). This puts strain on the heart and increases the risk of clotting or stroke.
Lipid Panel
What it is: A measurement of the fats in your blood.
The TRT Focus: TRT notoriously lowers HDL (the “Good” Cholesterol).
Why it matters: Testosterone speeds up the liver’s processing of cholesterol. While it might lower your LDL (Bad Cholesterol), if it crushes your HDL too low, you lose cardiac protection. You need to watch the ratio of Total Cholesterol to HDL to ensure long-term heart health.
Testosterone, Free & Total
Total Testosterone: The total amount of hormone floating in your bloodstream.
Free Testosterone: The amount of hormone that is actually unbound and available for your receptors to use.
Why it matters: You can have high Total T but feel terrible because your Free T is low (meaning it’s all locked up by binding proteins). You need both numbers to get the full picture.
Estradiol E2 (Sensitive)
What it is: The primary form of Estrogen in men.
The “Sensitive” Requirement: You must specifically request the “Ultrasensitive” or “LC/MS” (Liquid Chromatography/Mass Spectrometry) assay.
Why it matters: Standard estrogen tests are designed for women (who have high levels) and are inaccurate for men. A standard test often reads “Normal” even if you are actually high or low. The sensitive test provides the precision needed for male biology.
Prolactin
What it is: A peptide hormone produced by the pituitary that signals sexual satiety. It can increase when estrogen levels rise
The Process: You inject Testosterone—>Your body aromatizes (converts) some of it into Estrogen (Estradiol)—>High levels of Estrogen signal the pituitary gland to release more ProlactinWhy it matters: You can have elevated prolactin levels but normal range estrogen levels. High prolactin can kill libido and cause erectile dysfunction even if your testosterone is perfect. It is often elevated by stress or certain medications.
If you let your Estrogen get out of control, your Prolactin will often drift up with it.
Delayed Ejaculation (The #1 Tell): This is the specific hallmark of high prolactin. You can get an erection, you can have sex, but you physically cannot reach orgasm. It feels like the sensitivity has been turned down to 20%.
The Fix: Controlling estrogen will typically lower Prolactin as well. Sometimes Prolactin can be treated by an occasional dose of anti-prolactin drugs like Cabergoline, but this should always be assessed in context
PSA (Prostate-Specific Antigen)
What it is: A protein produced by the prostate gland.
The TRT Focus: Screening for prostate irritation or growth.
Why it matters: Testosterone converts to DHT, which can enlarge the prostate. While TRT does not cause prostate cancer, it can fuel existing issues.
The Red Flag: You aren’t just looking at the number (e.g., staying under 4.0 ng/mL); you are looking at the velocity. If it jumps from 1.0 to 2.5 in six months, that is a major warning sign, even if 2.5 is technically “safe.”
7. SHBG (Sex Hormone Binding Globulin)
What it is: The protein bus that transports testosterone around the body.
The TRT Focus: It dictates your injection frequency.
Why it matters:
High SHBG: It “steals” your testosterone, lowering your Free T. You may need a higher dose to feel benefits.
Low SHBG: Your body burns through testosterone very fast. You will likely need to inject more frequently (e.g., every other day rather than once a week) to keep levels stable.
Ferritin (optional)
What it is: A protein that stores iron inside your cells.
The TRT Focus: This is the check-and-balance for blood donation.
Why it matters: If your Hematocrit (from the CBC) gets too high, the standard treatment is to donate blood.
Summary Checklist for Blood Work
CBC (includes Hematocrit & Hemoglobin)
CMP (includes Liver & Kidney function)
Lipid Panel
Testosterone, Free & Total
Estradiol (Sensitive)
Prolactin
PSA
SHBG
Ferritin (if you donate blood)
I’d Recommend using the TRT panel from Vanguard labs to manage your health (use code AJAC10)
Diet and Training While on TRT
Combining TRT with a “bodybuilder lifestyle” is mandatory for health and results.
This is the biggest advantage of TRT. On TRT, your body preferentially shuttles nutrients into muscle tissue rather than fat cells. Your body has greater response to stimulus with liftig weights. You will build muscle and burn fat simultaneously (recomposition) at a rate that is difficult for natural trainees to match if you are intense with your training and disciplined with your eating.
There is no special kind of “TRT diet and exercise”. You follow the principles Ive written about many times over

8) The Most Common TRT Questions
So…how do I get TRT?? Can I buy it somewhere??
If you are asking this, I'm assuming you didn't read anything the article said and are an imbecile.
Could I just get testosterone and inject myself and do my own TRT?
The legality of this aside, I strongly DO NOT recommend trying to figure out your own hormones without medical supervision and blood tests.
The facts of that matter is that getting “dialed in” on TRT is not an overnight experience. To again reference past points, it will take a few weeks to notice effects, fluctuations in estrogen are common, you WILL need to get bloodwork done regularly to make sure all your numbers are in healthy range, and until you become familiar with terminology and have a basic 101 understanding of the science involved, the whole process is going to be unknown and somewhat intimidating. Working with an experienced physician makes it all much easier.
Do I need to automatically take Anti-estrogens if I'm on TRT?
You do not. In the past 5 years, the evidence has demonstrated that anti-estrogens are detrimental to cardiovascular health, and the usage of them to prevent gynecomastia is outweighed by their negative effects on heart health. It's still common practice to prescribe aromatase-inhibitors, but their usage is contextual.
This no doubt will cause confusion, as conventional practice for the last 30 years has led men to believe that their estrogen levels could spike, they could get gynecomastia, and that estrogen in general is BAD and must be avoided at all costs.
All of these beliefs have been proven largely untrue.
The Truth About Estrogen When using Therapeutic Testosterone
Your goal when on TRT is finding your own sweetspot for your estrogen levels, and only using AIs when needed.
Will I get Gynecomastia (bitch tits) if I take TRT?
About half of men are predisposed to Gyno. This could simply be gaining weight in the chest area and getting puffy looking nipples, to the development of full on breast tissue that is swollen, itchy, and painful.
Whether you get Gyno or not is entirely genetic. Ive known hardcore bodybuilders who used anabolic steroids for years, and never had gyno.
I've known natural trainees who had gyno simply from being overweight when they were young and it led to the dreaded “bitch tits”.
While using anabolic hormones can potentially lead to Gyno, whether you experience it or not is part genetically determined, and part how you manage your TRT (estrogen and prolactin)
Will my Hair fall out if I'm on TRT?
This is highly genetic and lifestyle driven. If you are 40+ and have not experienced any serious hair loss, it's likely you won't have to worry about hair loss from TRT.
If you started losing your hair at 20 though…yes, TRT is likely to speed that up.
I would suggest watching Derek's videos (More Plates More Dates) on what can be done to prevent hair loss while using TRT.
Will my Balls Shrink if I'm On TRT?
Yes, there will be testicular atrophy if you use testosterone by utself. That is a side effect of exogenous testosterone. This can be counteracted with HCG, which will maintain testicular fullness and function.
Will I roid rage on TRT?
No. You are likely to feel increased positivity and enjoyment from socializing versus being low T and estrogenic.
Roid rage is largely a media myth, and the aggressive irritability that supposedly happens is something that exists in the realm of the most extreme steroid users taking multiple grams of multiple compounds.
I’m 21/22/23/24 etc and I think my testosterone is Low, Can I get TRT???
Very unlikely unless your total levels were sub 300 and natural interventions in lifestyle change did absolutely nothing. It's highly probable you can increase your natural production without TRT.
I'm scared of needles, what other choices do I have?
As already mentioned, testosterone gels and creams exist, although they do not work as well as testosterone injections.
And as said prior, testosterone injections are quite easy to administer. They are done intramuscular (into muscle) or subcutaneously (into fatty dermal layers of the skin), you can often use insulin needles (which are very small), and whatever irrational fear you have about it, the actual experience is easy.
Will I get acne on TRT?
Acne is probably the most common side effect experienced by men who used anabolic steroids, whether it be for TRT doses or supraphysiological doses.
The possibility of getting acne depends on your genetic predisposition for acne, as well as your diet and overall lifestyle.
By my bro observations, whether someone gets acne or not seems to fall under a Bell curve distribution. Some men never get it, some men do, and some men get it really bad. If you are already predisposed for acne, it's possible that TRT could cause it to flare up.
That said, the severity of the acne tends to correspond with the dosages. The worst acne breakouts I've seen are in heavy steroid users who are also using estrogen suppressors too often.
A TRT dosage is typically too low to cause serious acne side effects in the majority of men. If there are some breakouts, they usually subside when the body adjusts to TRT and your estrogen levels stabilize, and your skin health usually improves.
You may experience some small breakouts, but it is manageable. Diet and hygiene and skincare play a major role. If you eat an optimized diet of non-inflammatory foods, and you shower regularly and use a good skin cleanser, it's unlikely you are going to experience massive bacne.
Will TRT give me Prostate Cancer? And a Heart attack? My doctor said I’ll get cancer and a heart attack. And DIE.
There is always a dramatic reaction whenever testosterone or anabolics in general are brought up in any public forum. The public has been misled for years that anabolics are extremely risky, they cause roid rage, and you’ll die from them within a short period of time. Steroids apparently are made by criminals capturing demons in hell and extracting their blood to turn men into muscle bound psychos with high blood pressure (Honestly demon blood would be cool as hell, but that is besides the point).
My point being, the emotional reactions people have are rarely (if ever) grounded in factual evidence.
Relative to TRT and the Therapeutic use of testosterone, TRT is far safer than people believe, and many of the supposed risks surrounding its usage have never been conclusively proven or even supported by the actual medical data.
The confusion surrounding TRT and Heart health is similar to the confusion surrounding TRT and Prostate health, it is applying monocausal thinking to a polycausal problem set.
Or said more simply,
Health is complicated, and there are multiple factors that affect things. If you don't account for this, your studies and your evidence are probably not going to be very useful, and could be very misleading,
Based on the current medical evidence, this “bad for you” argument is harshly contradicted by the following points of research that
-Testosterone DEFICIENCY increases likelihood of metabolic disease, diabetes, and cardiovascular risk.
-Testosterone improves metabolic health and insulin sensitivity in people with metabolic syndrome and diabetes
-There is no evidence that Testosterone therapy causes prostate cancer
-Testosterone CAN be safely used to treat men who are hypogonadal and have prostate cancer
-Testosterone deficiency is a risk factor for cardiovascular disease 1
-testosterone deficiency is a risk factor for cardiovascular disease 2
-Testosterone deficiency is a risk factor for cardiovascular disease 3
I could keep going with this for a while. One can say I'm cherry picking studies, but all of these studies are from the past 10 years, and this is not an exhaustive list by any means.
The overall consensus is clear that the past fear-mongering of TRT being a causative agent of heart attacks and prostate cancer is largely unfounded, and the evidence contextually suggests almost the exact opposite; TRT is safe to use and can improve both of these conditions.
All of the most recent evidence of the past decade either renders Null the arguments of therapeutic testosterone being dangerous and high risk.
Can I stop TRT? Or do I need to be on it for Life?
TRT is usually a lifelong treatment. Sometimes men stop it when they want to conceive with their wife and restore their fertility to full power, and then they get on again.
If the idea of being on TRT for life is distasteful to you, so it is. Your health decisions are ultimately your own.
Should I go on TRT if I am overweight/obese?
One of the major issues with prescribing TRT and its associated risks is whether the men in need of it are HEALTHY to begin with.
There are multiple confounding factors at play, the main ones being
-men are who are obese are at higher risk for cardiovascular events
-men with high blood pressure
-men who do not exercise are at higher risk
But these men also are MORE likely to be testosterone deficient.
Based on the current evidence, testosterone therapy CAN be safe, but your individual risk profile needs to be assessed. If you are severely obese, losing bodyfat first is probably advisable before embarking on TRT.
Does TRT make you Infertile forever? Will I be shooting blanks and never be able to have children?
No. This is another myth that the public has been misled about for years.
Speaking personally, I've had a number of friends who were on supraphysiological doses of testosterone and other steroids, and they inadvertently got their wives or girlfriends pregnant.
This directly defies the idea that exogenous testosterone cancels you out entirely.
That said, do not take that to mean that TRT keeps you fertile (clearly it does not) or isn't a big deal.
Taking exogenous testosterone does MOSTLY shutdown sperm production, but not entirely.
But this shutdown is not permanent. Fertility can be restored through the usage of HCG (or by simply going off TRT entirely)
TRT also has different effects on different men. Sperm count, sperm motility, and sperm morphology are all different factors.
Most men their sperm count simply declines, but other men their sperm's ability to swim, or the structure of the sperm itself, is affected.
If you are on TRT and you decide you want to have kids, you need to get your sperm tested.
Data>Speculation.
HCG is usually the first course of treatment.
HCG increases sperm production, even while on TRT
Taking HCG and TRT together is popular for this reason.
If taking HCG is not enough, its likely a doctor would advise you to go off of TRT entirely, to allow your natural production to fully takeover
Even the Most HARDCORE steroid users can restore their fertility
Obviously he is not a physician, but this is one area of medicine where the Bros have more insight and anecdotal evidence than the clinicians do.
I started taking TRT but now my blood pressure went up and I'm not getting lean how I thought I would and my doctor is concerned saying I need to stop, why did this happen?
First question: ARE YOU WORKING OUT AND EATING CLEAN?
For reasons unknown to me, there is always a segment of men who do not lift weights or workout regularly, do not do cardio, do not eat a healthy diet…but they decide to use testosterone (whether it be therapeutic or supraphysiological).
And then they are surprised when they dont turn into Captain America. It is baffling.
If you want to maximize the effects of TRT, you should be
-Eating a whole foods, nutritious diet
-Lifting weights regularly and training to get stronger
-Doing regular cardio, especially as you age
If you are not doing any of that, and then you are surprised that TRT does not instantaneously transform your body, you are fucking up.
Second question: Are you having blood work done and keeping your testosterone within healthy high normal levels, or are you taking too high of a dose?
This is why regular blood work is needed.. If your dosage of T is too high, YES, it may elevate biomarkers like blood pressure or LDL holesterol.
Getting the dosage right is critical. The goal is to optimize, not dose to excess. Start conservative with your dosage, be it injectables, gels, or creams.
Third question: are you taking an AI (aromatase inhibitor)
AIs are notorious for making men feel like shit while also wrecking HDL levels and have an overall negative effect on cardiovascular markers.
To self-reference again: You should not be immediately blocking estrogen when you start TRT
what is your opinion on DHEA? Taking 50mg a day since years with good results, I am 56 years old...